
Pelvic Organ Prolapse: The Condition No One Talks About
Millions of women live with a condition that affects their daily life, their confidence, and their body - and most of them have never heard it named. Pelvic organ prolapse is one of the most common yet least discussed women's health issues in the world. If you've ever felt pressure "down there," noticed something bulging, or been told your bladder has "dropped," you may already know what this feels like. You just may not have known what to call it - or that help exists.
This guide breaks down everything you need to know about pelvic organ prolapse: what it is, why it happens, how it feels, and - most importantly - what you can do about it.
What Is Pelvic Organ Prolapse?
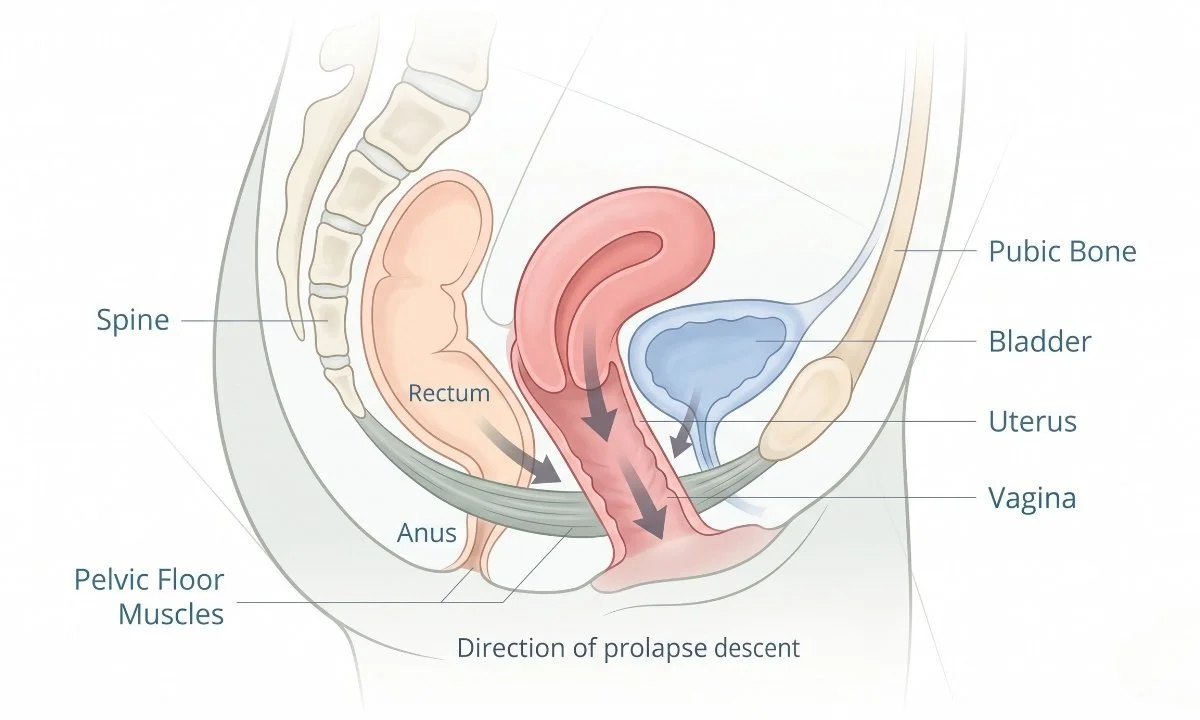
Pelvic organ prolapse (POP) occurs when the muscles and connective tissues of the pelvic floor weaken or stretch to the point where they can no longer support the pelvic organs - the bladder, uterus, rectum, or small bowel. When this support fails, one or more of these organs can descend into or even outside the vaginal canal.
It's not a rare condition. Research suggests that up to 50% of women who have given birth have some degree of prolapse, though many never experience noticeable symptoms. Among those who do experience symptoms, fewer than 20% seek treatment - largely because of embarrassment, lack of awareness, or the mistaken belief that it's simply a normal part of aging.
It is common. It is not something you have to accept as your new normal.
Types of Pelvic Organ Prolapse
There are several distinct types, each named for the organ that has descended:
Cystocele (Anterior Prolapse): The bladder drops into the front wall of the vagina. This is the most common type.
Rectocele (Posterior Prolapse): The rectum bulges into the back wall of the vagina.
Uterine Prolapse: The uterus descends into the vaginal canal.
Vault Prolapse: After a hysterectomy, the top of the vagina can drop inward.
Enterocele: The small intestine pushes against the upper portion of the vagina.
Many women experience more than one type simultaneously, which is why an accurate diagnosis from a healthcare provider is essential before beginning any treatment plan.
Who Is at Risk? Understanding the Causes of Pelvic Organ Prolapse
Pelvic organ prolapse doesn't happen overnight - it develops over time as the result of accumulated stress on the pelvic floor. Understanding the root causes can help you identify your own risk factors and take proactive steps.
Childbirth and Pregnancy
Vaginal delivery is one of the most significant risk factors for POP. Prolonged pushing during labor, large babies, the use of forceps or vacuum assistance, and multiple deliveries all increase the strain placed on the pelvic floor muscles and fascia. Even women who deliver by cesarean section are not entirely without risk, as pregnancy itself places sustained downward pressure on pelvic structures for nine months.
Hormonal Changes and Menopause
Estrogen plays a crucial role in maintaining the strength and elasticity of pelvic floor tissues. As estrogen levels decline during perimenopause and menopause, the connective tissue supporting the pelvic organs becomes less resilient. This is why many women first notice prolapse symptoms in their 50s and 60s, even if the underlying weakness began years earlier.
Chronic Pressure on the Pelvic Floor
Anything that repeatedly increases intra-abdominal pressure can accelerate prolapse. This includes:
Chronic constipation and straining during bowel movements
Chronic cough from smoking or respiratory conditions
Heavy lifting without proper intra-abdominal pressure management
Obesity, which places constant downward load on pelvic structures
Genetics and Connective Tissue Disorders
Some women are simply born with naturally looser connective tissue. Conditions like hypermobility syndrome or a family history of prolapse significantly increase susceptibility. If your mother or sister has experienced POP, your own risk is higher than average.
Recognizing the Symptoms: What Pelvic Organ Prolapse Feels Like
One of the reasons pelvic organ prolapse goes undetected for so long is that the symptoms are often vague, fluctuating, and easy to dismiss. Symptoms tend to be worse at the end of the day, after long periods of standing, or after physical exertion - and may feel better after lying down.
Common Physical Symptoms
Symptom
What It Might Feel Like
Pelvic pressure or heaviness
A feeling that something is "falling out" or a constant dragging sensation
Visible or palpable bulge
A soft lump at or outside the vaginal opening
Bladder dysfunction
Urinary leakage, difficulty emptying fully, or frequent urgency
Bowel dysfunction
Constipation, incomplete emptying, or needing to splint (use fingers to assist)
Sexual discomfort
Pain or reduced sensation during intercourse
Low back ache
Dull, persistent ache in the lower back or pelvis
Grading the Severity
Healthcare providers use the POP-Q staging system to grade prolapse severity from Stage 0 (no prolapse) to Stage IV (complete prolapse beyond the vaginal opening). Many women with Stage I or II prolapse have no symptoms at all. Symptoms typically become noticeable at Stage II and beyond.
It's worth noting that the degree of anatomical prolapse does not always correlate with how severely a woman feels it. Some women with Stage III prolapse report minimal discomfort, while others with Stage II are significantly affected. Your symptoms matter more than a number on a chart.
How Pelvic Organ Prolapse Is Diagnosed
If you suspect you may have a prolapse, the first step is speaking with your physician or a pelvic health physiotherapist. Diagnosis is typically straightforward and involves:
A thorough health history - reviewing your pregnancies, surgeries, bowel and bladder habits, and symptoms
A physical (pelvic) examination - performed while you bear down (the Valsalva maneuver), which reveals the extent of descent
Urodynamic testing - sometimes ordered to assess bladder function if urinary symptoms are prominent
Imaging - ultrasound or MRI may be used in complex cases
You should never feel embarrassed discussing these symptoms with a healthcare provider. These professionals examine and treat pelvic floor conditions every day. The earlier a prolapse is identified, the more treatment options are available.
Pelvic Organ Prolapse Treatment: What Are Your Options?
The good news: pelvic organ prolapse is treatable, and in many cases, significant improvement is possible without surgery. Treatment is tailored to the type and grade of prolapse, your symptoms, and your personal goals.
Pelvic Floor Physiotherapy - The Foundation of Conservative Care
Pelvic floor physiotherapy is widely recognized as the first-line treatment for pelvic organ prolapse. A trained pelvic health physiotherapist assesses the strength, coordination, and endurance of your pelvic floor muscles and creates a personalized rehabilitation program.
This is not simply "doing Kegels." Effective pelvic floor rehabilitation involves:
Targeted muscle strengthening - progressive resistance exercises for the pelvic floor
Coordination training - learning to pre-contract the pelvic floor before moments of increased pressure (coughing, lifting, sneezing)
Postural and breathing work - correcting habitual postures and breathing patterns that increase intra-abdominal pressure
Bowel and bladder retraining - reducing straining habits that worsen prolapse over time
Research consistently shows that pelvic floor muscle training reduces prolapse symptoms in the majority of women and can even improve the anatomical position of the organs over time.
Pessary Devices
A pessary is a small, removable silicone device inserted into the vagina to provide mechanical support to prolapsed organs. Pessaries are a non-surgical, reversible option that many women use long-term - particularly those who are not surgical candidates or who prefer to avoid surgery. They come in various shapes and sizes and must be fitted by a healthcare provider.
Lifestyle and Behavioral Modifications
Regardless of which treatment path you choose, certain lifestyle changes are universally recommended:
Managing constipation through adequate fibre, hydration, and correct toileting posture
Weight management to reduce chronic pelvic floor loading
Avoiding prolonged heavy lifting, or learning to lift with proper pressure management techniques
Quitting smoking to reduce chronic cough
Surgical Treatment
Surgery is considered when conservative measures haven't provided sufficient relief and symptoms significantly impair quality of life. Common surgical approaches include pelvic floor repair (colporrhaphy) and sacrocolpopexy. Surgery carries risks and is not necessary for all women with prolapse - a thorough discussion with a urogynecologist is essential before making this decision.
The Role of Exercise: What's Safe and What to Avoid

If you have pelvic organ prolapse, you don't need to stop exercising. But you do need to exercise smarter. High-impact, high-load activities performed without proper pelvic floor preparation can worsen symptoms or slow recovery.
Exercises Generally Safe with POP
Walking and swimming
Low-impact yoga and Pilates (with modifications)
Cycling on a recumbent bike
Resistance training with appropriate load management and breathing technique
Exercises to Approach with Caution
Heavy barbell lifting (especially if symptoms worsen during or after)
High-impact running and jumping (especially without pelvic floor coordination)
Activities that cause leakage or a feeling of increased heaviness
The goal is not to avoid movement - it's to build a body that can manage pressure and load without letting it escape downward. This is exactly the kind of personalized guidance that fitness professionals with pelvic health expertise can provide.
Living with Pelvic Organ Prolapse: The Emotional Side
Pelvic organ prolapse doesn't just affect the body. Many women describe feelings of shame, embarrassment, loss of confidence, and grief over changes to their body - particularly around sexuality and physical capability.
These feelings are valid. And they are also not permanent.
Women who engage in active treatment - whether through pelvic floor physiotherapy, guided exercise, or a combination of approaches - report significant improvements not only in physical symptoms but in body confidence, sexual satisfaction, and overall quality of life.
You are not broken. Your body has done extraordinary things. It deserves knowledgeable, compassionate care.

Frequently Asked Questions About Pelvic Organ Prolapse
Can pelvic organ prolapse heal on its own without treatment?
Mild prolapse (Stage I) may not worsen over time, especially if you avoid aggravating factors and maintain pelvic floor strength. However, prolapse does not typically resolve on its own without targeted intervention. Pelvic floor physiotherapy is the most evidence-based conservative approach and can produce meaningful improvements - but the prolapse is unlikely to disappear without some form of active management.
Is it safe to exercise with pelvic organ prolapse?
Yes - in most cases, exercise is not only safe but beneficial. The key is choosing appropriate activities and learning to manage intra-abdominal pressure correctly. A pelvic health physiotherapist or a fitness professional trained in pelvic floor dysfunction can help you identify which exercises are appropriate for your current stage of prolapse and your symptoms.
Will I need surgery for pelvic organ prolapse?
Not necessarily. Many women with prolapse manage their symptoms very successfully through conservative treatment alone - particularly pelvic floor physiotherapy, pessary use, and lifestyle changes. Surgery is typically reserved for cases where conservative treatment has not provided adequate relief and where symptoms are significantly affecting quality of life. The decision should always be made collaboratively with your healthcare team.
Can pelvic organ prolapse come back after surgery?
Unfortunately, yes. Prolapse recurrence rates after surgery vary depending on the type of repair and individual factors, but recurrence is a known risk. This is one of the reasons pelvic floor physiotherapy is recommended both before and after surgical repair - building strong, well-coordinated pelvic floor muscles reduces the likelihood of recurrence.
Can younger women get pelvic organ prolapse?
Yes. While prolapse is more common in perimenopausal and postmenopausal women, it can and does occur in younger women - particularly those who have had vaginal deliveries, have connective tissue laxity, or engage in high-load physical activity without adequate pelvic floor support. Age is a risk factor, but it is not a prerequisite.
Conclusion
Pelvic organ prolapse affects millions of women - and the silence around it has gone on far too long. Whether you're experiencing subtle symptoms or have been living with significant discomfort, the most important thing to know is this: you have options, you are not alone, and effective help exists.
From pelvic floor physiotherapy to guided exercise programming to medical management, there are multiple pathways to living a full, active, symptom-free life with - or after - a prolapse diagnosis. The first step is simply talking about it.
At Anchor Health and Fitness Centre, we work with women at every stage of their pelvic health journey. Whether you're recovering postpartum, navigating perimenopause, or returning to exercise after a prolapse diagnosis, our team is here to help you move with confidence and strength.Book a consultation with our team today and take the first step toward reclaiming your pelvic health.